Arthritis in Dogs: Symptoms, Stages, and Treatment Options That Actually Work
December 22, 2023 | by seniorsniffs.com

Arthritis in Dogs: Symptoms, Stages, and Treatment Options That Actually Work

Your dog used to bound up the stairs. Now there is a pause at the bottom, a slow stretch, a careful first step. That hesitation is one of the earliest signs of a disease that affects roughly one in five adult dogs. The good news: modern veterinary medicine has changed dramatically in the last five years, and a stiff dog today has more effective treatment options than at any point in history.
Arthritis in dogs, more accurately called osteoarthritis (OA), is a progressive degenerative joint disease in which the cartilage cushioning the bones inside a joint breaks down faster than the body can repair it. The result is inflammation, pain, reduced range of motion, and bony changes around the joint. OA is chronic, but with the right plan it is highly manageable.
This guide walks through every stage of the disease, the symptoms to watch for, how vets diagnose it, and which treatments have strong clinical evidence behind them, including the new monoclonal antibody therapies that have transformed care since 2023.
How Common Is Arthritis in Dogs?
Canine osteoarthritis is one of the most common chronic diseases in companion animals. Roughly 20 percent of dogs over one year old will show signs of OA during their lifetime, and that figure climbs to about 80 percent in dogs aged eight years and older, according to the Cornell University College of Veterinary Medicine. Translated into real numbers: tens of millions of dogs in North America alone are living with arthritic joint changes right now.
Here is the statistic most owners never hear. A 2024 study published in Scientific Reports examined dogs aged 8 months to 4 years and found that 39.8 percent already had radiographic osteoarthritis in at least one joint. Of those, 40 to 60 percent had clinically detectable pain. The takeaway is sobering. OA is not just an old-dog disease. It can begin silently in puppyhood, particularly in large breeds with developmental orthopedic conditions, and most cases are not diagnosed until the dog is between five and thirteen years old. By then, the cartilage damage is well established.
The clinical message from VCA Animal Hospitals and other major veterinary networks is consistent: OA is underdiagnosed, undertreated, and very rarely caught early. Owners and clinicians both tend to interpret early stiffness as “slowing down with age,” when in fact it is a treatable inflammatory disease in its first stage.
Signs of Arthritis in Dogs
Dogs are masters at hiding pain. Pack instinct, stoicism, and the simple fact that they cannot tell you their hip hurts means owners must learn to read subtle behavioral shifts. The signs of arthritis in dogs fall into two categories: behavioral changes and physical changes. Behavioral signs almost always appear first.
Early behavioral signs
- Reluctance to jump onto the couch, bed, or into the car
- Slower to rise after lying down, especially first thing in the morning
- Lagging behind on walks or wanting to turn back early
- Reduced enthusiasm for play, fetch, or stair climbing
- Changes in sleeping position or trouble settling
- Increased irritability, especially when touched on the hips, shoulders, or spine
- Excessive licking of one joint or area
- Subtle changes in posture, such as a roached back or shifted weight
Advanced and physical dog arthritis symptoms
- Visible lameness or limping, often worse after rest and improving with light movement
- Muscle atrophy over the hips, shoulders, or thighs
- Audible joint crepitus (clicking or grinding sounds) during movement
- Reduced range of motion on physical examination
- Swollen joints or palpable thickening of the joint capsule
- Difficulty squatting to urinate or defecate
- Knuckling, paw dragging, or worn nails on one side from altered gait
- Weight gain secondary to inactivity, which then accelerates the cycle
One of the most useful tells, described by Texas A&M College of Veterinary Medicine, is the “warm-up shuffle.” An arthritic dog is often stiffest after rest. The first few steps look painful, but the gait loosens as the joints warm up with movement, only to stiffen again after the next rest. If you see this pattern, do not wait. Make a vet appointment.
The Four Stages of Canine Osteoarthritis
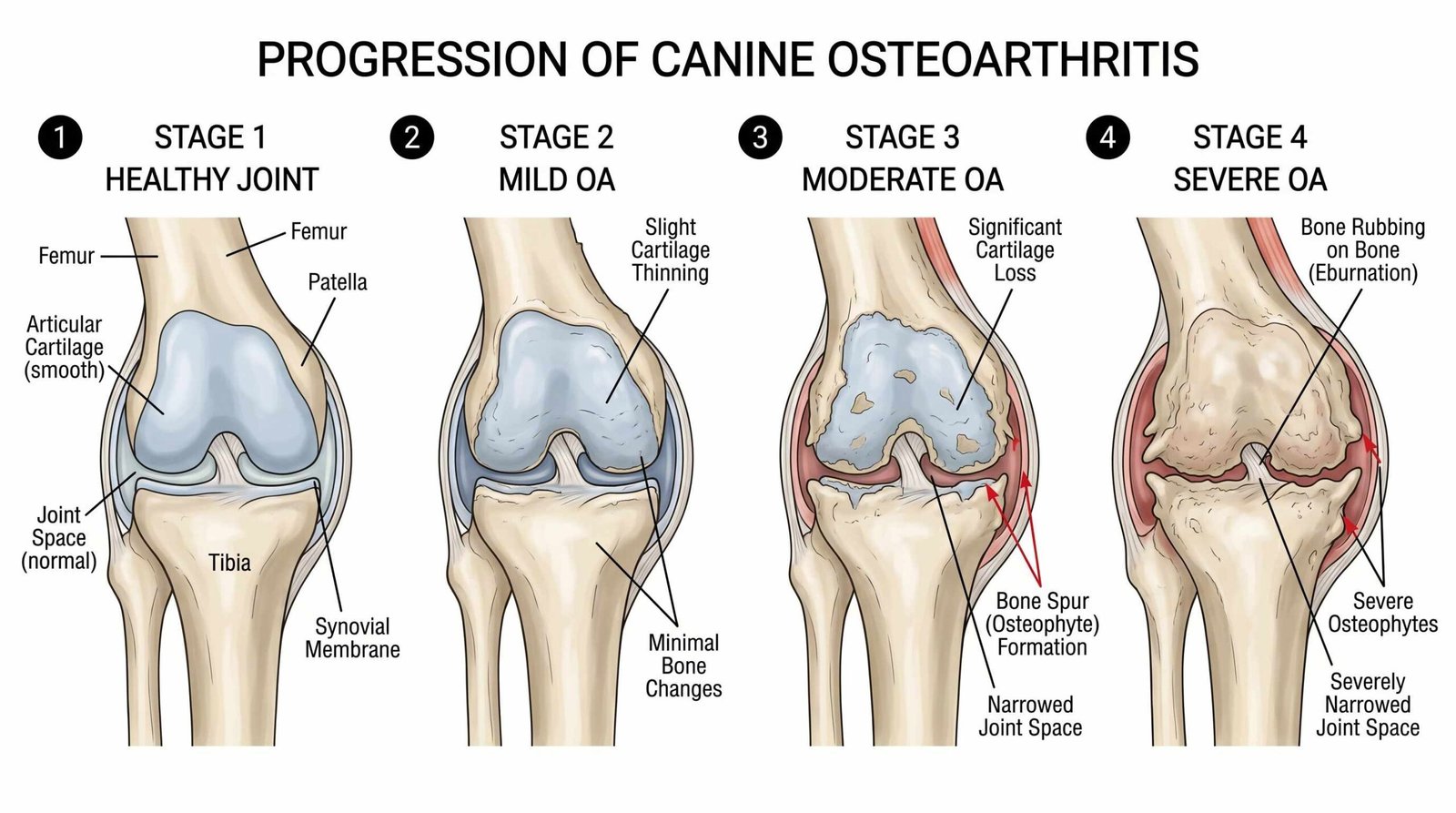
One of the most useful clinical tools developed in the last decade is the Canine OsteoArthritis Staging Tool (COAST), created by an international group of veterinary specialists. COAST classifies dogs on a 0 to 4 scale, integrating risk factors, owner observations, physical examination, and radiographs. Knowing your dog’s stage tells you what to expect, what to monitor, and which treatments are appropriate. Below is a practical translation of the four stages most owners encounter.
Stage 1: Preclinical, at-risk dog
The dog appears clinically normal but carries one or more risk factors: a predisposed breed, history of joint injury, overweight body condition, repetitive high-impact activity, or developmental conditions like elbow or hip dysplasia in dogs. Radiographs may already show very early changes even though the dog runs and plays normally. This stage is where prevention pays off the most. Weight optimization, joint-supportive nutrition, and controlled exercise can delay clinical disease by years.
Stage 2: Mild OA
Now the dog shows mild clinical signs, but they are easy to miss. Slight stiffness after rest, mild reluctance to jump, slower on the second half of a long walk. Radiographs show early osteophyte (bone spur) formation and mild joint space narrowing. Treatment at this stage is typically multimodal but conservative: weight management, controlled exercise, omega-3 fatty acid supplementation, and short courses of NSAIDs or grapiprant during flare-ups.
Stage 3: Moderate OA
Clinical signs are consistent and obvious. The dog is lame after rest, struggles with stairs, has reduced muscle mass, and shows clear discomfort on joint palpation. Radiographs show significant osteophytes, sclerosis of subchondral bone, and visible joint space narrowing. This is the stage where most dogs are first diagnosed, which is unfortunate because earlier intervention is more effective. Daily multimodal therapy is the standard: NSAIDs or grapiprant, anti-NGF monoclonal antibody injections, weight optimization, formal physical rehabilitation, and adjunctive analgesics as needed.
Stage 4: Severe OA
The dog has marked functional impairment. Lameness is persistent, range of motion is severely limited, and quality of life is affected. Radiographs show advanced bone remodeling, enthesophytes, possible joint subluxation, and substantial joint space loss. Treatment requires aggressive multimodal management combining NSAIDs, biologics like bedinvetmab, gabapentin or amantadine for neuropathic pain components, strict weight control, structured rehabilitation, and consideration of interventional options including intra-articular therapies, regenerative medicine, or surgical procedures such as joint replacement or arthrodesis.
Staging matters because each step up the ladder usually requires adding tools, not switching them. A dog at Stage 3 still benefits from the foundational weight and exercise work that started at Stage 1.
Causes and Risk Factors
Osteoarthritis develops when something disturbs the normal balance of cartilage maintenance and repair inside a joint. The root causes fall into several overlapping categories.
Breed predisposition
Genetics matter enormously. Large and giant breeds carry the highest baseline risk because of the mechanical loads on their joints and because of breed-specific orthopedic conditions. Breeds most predisposed to OA include:
- Labrador Retrievers and Golden Retrievers, which are prone to hip and elbow dysplasia and cranial cruciate ligament disease
- German Shepherds, with high rates of hip dysplasia and degenerative myelopathy that compounds mobility loss
- Rottweilers, Bernese Mountain Dogs, and Newfoundlands, which combine large frames with developmental orthopedic disease
- Mastiffs and Great Danes, where sheer body weight stresses joints
- Bulldogs and French Bulldogs, with conformational issues that predispose them to elbow and shoulder OA
- Dachshunds and Corgis, where the long-back, short-leg conformation drives spinal and stifle OA
- Cocker Spaniels and Springer Spaniels, with high rates of hip dysplasia
Body weight
Excess weight is the single most modifiable risk factor. Adipose tissue is not inert. It secretes inflammatory cytokines that worsen joint inflammation, on top of the mechanical strain of extra pounds. A landmark Labrador Retriever lifetime study showed that dogs kept lean lived nearly two years longer and developed clinically detectable OA roughly two years later than their littermates fed 25 percent more food.
Prior injury and developmental conditions
Any joint that has been injured will likely develop OA over time. Cranial cruciate ligament rupture is the most common driver of stifle OA in dogs, and even with surgical repair, OA progression is almost universal. Developmental orthopedic diseases, including hip dysplasia, elbow dysplasia, osteochondritis dissecans (OCD), and patellar luxation, set the joint up for accelerated cartilage wear.
Age and activity
Cumulative wear matters, but so does the type of activity. Repetitive high-impact work (agility, flyball, sustained running on hard surfaces) accelerates OA, particularly in dogs with subtle conformational issues. Sedentary dogs are not protected either. Lack of muscle mass leaves joints unsupported and contributes to the cycle.
How Vets Diagnose Arthritis
Diagnosing OA is rarely a single test. It is a clinical picture assembled from history, examination, and imaging. A thorough workup typically includes the following.
History and owner questionnaires
Your vet will ask detailed questions about onset, daily patterns, exercise tolerance, behavioral changes, and which activities have become harder. Two validated owner-completed pain scoring tools have made this conversation much more rigorous: the Helsinki Chronic Pain Index and the Liverpool Osteoarthritis in Dogs (LOAD) scale. Both ask owners to rate mobility, demeanor, and lameness on standardized items. We suggest filling out one of these scales before your appointment, then repeating it every few months to track response to treatment. They turn a vague impression (“she seems a bit better”) into a number you can actually follow.
Physical and orthopedic examination
A skilled vet will watch your dog walk and trot, palpate every joint for swelling, heat, or pain response, manipulate each joint through its range of motion, and check for muscle atrophy by measuring thigh circumference. Crepitus on joint flexion, reduced range of motion, and pain on extension or flexion are hallmark findings.
Gait analysis
Specialty hospitals use force-plate gait analysis or pressure-sensitive walkway systems to objectively measure weight bearing on each limb. This is the gold standard for documenting subtle lameness and tracking treatment response, though it is not available at every practice.
Radiographs and advanced imaging
X-rays remain the workhorse imaging modality. Radiographic OA findings include osteophyte formation, subchondral bone sclerosis, joint space narrowing, intra-articular mineralization, and joint capsule thickening. Radiographs underestimate cartilage damage, however. CT and MRI are more sensitive but reserved for surgical planning or unusual cases. Joint fluid analysis can rule out infectious or immune-mediated arthritis when the clinical picture is atypical.
Treatment Options for Arthritis in Dogs
Modern OA care is multimodal. No single therapy controls the disease on its own. The most effective protocols combine pharmacologic, nutritional, physical, and environmental interventions, escalating as the disease progresses. Below is the current arthritis treatment dogs toolkit, organized by category.
Non-steroidal anti-inflammatory drugs (NSAIDs)
NSAIDs for dogs remain the backbone of arthritis pharmacotherapy. They reduce inflammation and pain by inhibiting cyclooxygenase (COX) enzymes. Canine-specific NSAIDs commonly prescribed include:
- Carprofen (Rimadyl, Novox), one of the most widely used, with decades of clinical data
- Meloxicam (Metacam), available in oral suspension and tablets
- Deracoxib (Deramaxx), a COX-2 selective option
- Firocoxib (Previcox), also COX-2 selective and labeled for chronic use
- Grapiprant (Galliprant), a piprant class drug that targets the EP4 prostaglandin receptor specifically, with a different gastrointestinal and renal safety profile than traditional NSAIDs
Never give human NSAIDs (ibuprofen, naproxen, aspirin) to dogs. They are toxic at routine human doses and can cause severe gastrointestinal ulceration, renal failure, and death. NSAIDs require baseline and periodic bloodwork to monitor liver and kidney function. Your vet will determine the appropriate dose for your dog’s weight, age, and bloodwork results.
Biologic therapy: bedinvetmab (Librela)
Bedinvetmab, marketed as Librela by Zoetis, is a canine monoclonal antibody that binds and neutralizes nerve growth factor (NGF). NGF is elevated in arthritic joints and amplifies pain signaling. Approved by the FDA in May 2023, bedinvetmab is given as a once-monthly subcutaneous injection. It does not require liver or kidney metabolism, which makes it attractive for older dogs with comorbidities that limit NSAID use. The AKC Canine Health Foundation describes this drug class as the most significant advancement in canine OA pain management in a generation.
Clinical trials show meaningful improvements in pain interference, pain severity, and quality of life scores. Post-marketing surveillance has raised concerns about rare adverse events including neurological signs and reports of rapidly progressive osteoarthritis (RPOA) in some patients. We suggest discussing the full risk-benefit picture with your vet, especially if your dog has comorbid neurological disease.
Gabapentin and other adjunctive analgesics
Gabapentin for dogs is widely used as an adjunct in moderate to severe OA, particularly when there is a suspected neuropathic component to the pain. It is not a first-line therapy but layers well with NSAIDs or bedinvetmab. Amantadine, a NMDA receptor antagonist, is another adjunct that can address central sensitization in chronic pain. Tramadol was historically prescribed but recent evidence suggests poor analgesic efficacy in dogs for chronic OA pain, so it has fallen out of favor as a primary option.
Weight management
If your dog is overweight, the single highest-impact intervention is a structured weight loss plan. Research consistently shows that dogs who lose even a modest amount of excess body weight have measurable improvements in lameness scores, often equivalent to what a course of NSAIDs would deliver. The mechanism is twofold: less mechanical load on the joints and less systemic inflammation from adipose tissue. We suggest a vet-supervised plan rather than DIY calorie restriction, because muscle preservation is essential.
Physical rehabilitation and hydrotherapy
Veterinary physical rehabilitation is an underused but evidence-supported pillar of OA care. A certified canine rehab therapist (CCRT or CCRP) can design a program of therapeutic exercises, range-of-motion work, manual therapy, and modalities like therapeutic ultrasound or laser. Underwater treadmill therapy, often called hydrotherapy, is especially valuable. Buoyancy reduces joint loading while warm water relaxes muscles, allowing the dog to build strength and range of motion with minimal pain.
Acupuncture
Veterinary acupuncture has accumulated a modest but real body of evidence for chronic OA pain. Studies are limited and heterogeneous, but several controlled trials show measurable improvements in pain scores and gait. It is not a replacement for pharmacologic management, but as an adjunct in a multimodal plan it is reasonable to consider.
Emerging and interventional therapies
Synovetin OA is an intra-articular injection of tin-117m, a radioactive isotope that delivers low-energy electron radiation directly to the inflamed synovium. It is currently labeled for elbow OA in dogs. A single injection can provide approximately one year of pain relief in appropriate candidates. Intra-articular platelet-rich plasma (PRP) and stem cell injections have growing but still mixed evidence. Peripheral nerve blocks, including pulsed radiofrequency procedures, are being explored at referral centers for refractory cases. Surgical options including total hip replacement and arthrodesis remain appropriate for end-stage disease in specific joints.
Arthritis Treatment Options at a Glance
| Treatment | Best For | Evidence Level | Notes |
|---|---|---|---|
| NSAIDs (carprofen, meloxicam, firocoxib, deracoxib) | Mild to severe OA, daily pain control | Strong | Requires baseline and ongoing bloodwork |
| Grapiprant (Galliprant) | Dogs with mild-to-moderate OA, older dogs, GI or renal sensitivity | Strong | EP4 receptor antagonist, different safety profile |
| Bedinvetmab (Librela) | Moderate to severe OA, dogs intolerant of NSAIDs | Strong, with ongoing pharmacovigilance | Monthly subcutaneous injection |
| Gabapentin | Adjunctive analgesia, neuropathic component | Moderate | Often layered with NSAIDs |
| Omega-3 fatty acids (EPA/DHA) | All stages | Good clinical evidence | Doses higher than general wellness ranges |
| Glucosamine/chondroitin | Adjunct only | Mixed/weak | Low-risk; do not rely on as monotherapy |
| Weight loss | Any overweight arthritic dog | Strong | High-impact, low-cost, vet-supervised plan |
| Physical rehabilitation/hydrotherapy | All stages, post-surgical | Moderate to strong | Find a CCRT/CCRP-certified therapist |
| Acupuncture | Adjunct in multimodal plan | Limited but real | Best paired with pharmacology |
| Synovetin OA | Elbow OA in eligible dogs | Emerging | Single injection, ~1 year duration |
Supplements for Canine Arthritis: What the Evidence Actually Shows
The supplement aisle is crowded, the marketing is loud, and the science is uneven. Here is an honest read on dog arthritis supplements graded by current clinical evidence.
Omega-3 fatty acids (EPA and DHA): good evidence
This is the most clinically validated dog joint supplement available. Two 2010 Roush et al. studies published in the Journal of the American Veterinary Medical Association demonstrated that dogs fed a diet enriched with fish-oil-derived EPA and DHA showed measurably improved weight bearing and reduced NSAID requirements compared to controls. A subsequent randomized, double-blind, placebo-controlled trial reported approximately 50 percent improvements in crepitus, pain, and joint effusion at day 42 in dogs receiving high-dose fish oil. Effective therapeutic doses are higher than general wellness ranges, typically in the range of 50 to 100 mg per kilogram of combined EPA and DHA per day. See our guide on fish oil for dogs for product quality considerations. Your vet will determine the appropriate dose for your dog.
Glucosamine and chondroitin sulfate: mixed evidence
This is the supplement most owners reach for first, and the evidence for it is honestly less robust than the marketing suggests. Some studies show modest improvements in clinical signs. Other well-designed trials find no statistically significant benefit over placebo. The biological rationale (providing substrate for cartilage matrix) is reasonable, the safety profile is excellent, and many vets still suggest a trial because the risk is low. We will not tell you it is useless. We will tell you not to rely on it as the centerpiece of treatment. If it helps, it helps as part of a multimodal plan.
CBD and hemp products: emerging, limited
CBD has generated enormous interest among owners. A small number of controlled trials, including studies from Cornell and Baylor, have shown statistically significant improvements in pain and activity scores in arthritic dogs receiving full-spectrum CBD at doses around 2 to 4 mg per kilogram twice daily. These are preliminary results from small studies. Product quality varies wildly because the supplement industry is poorly regulated. Some products contain less CBD than labeled, others contain detectable THC, which is toxic to dogs at sufficient doses. If you decide to try CBD, choose a veterinary-marketed product with a third-party certificate of analysis and discuss it with your vet, especially if your dog takes other medications.
Curcumin and turmeric: very limited clinical evidence
Curcumin has clear in vitro anti-inflammatory activity, but rigorous clinical trials in dogs with OA are sparse, and oral bioavailability is a known problem. We do not yet have the data to make a strong evidence-based case for routine use. It is reasonable in a multimodal plan, not adequate as a primary therapy.
Green-lipped mussel (Perna canaliculus)
Green-lipped mussel extract has shown modest improvements in clinical signs in a few controlled trials, including improvements in joint pain and mobility scores. The evidence is encouraging but not as robust as the omega-3 data. Many therapeutic joint diets already include it as part of a broader formulation.
We do not endorse specific brands. We do suggest choosing supplements that carry the NASC (National Animal Supplement Council) quality seal and that publish third-party testing results.
Home Management: Making Life Easier for an Arthritic Dog

The home environment is the most consistently underrated piece of OA management. Medication works for a few hours a day. Environment works twenty-four hours a day. Small modifications produce outsized quality-of-life gains.
- Eliminate slippery floors. Hardwood, tile, and laminate floors are a daily injury risk for arthritic dogs. Lay down area rugs, yoga mats, or runners along regular travel paths. Toe grips and traction socks can help on stubborn surfaces. Non-slip stair treads are essential on any wooden or tile staircase your dog uses.
- Install ramps. Jumping into the car, onto the bed, or onto the couch creates repeated high-impact stress on diseased joints. A sturdy ramp with a non-slip surface protects joints and lets your dog continue doing what they enjoy. See our reviews of ramps for dogs for guidance on choosing the right gradient and weight capacity.
- Upgrade the bed. A genuine orthopedic memory foam bed (not the marketing kind, the dense supportive kind, at least 4 inches thick) reduces pressure on hips, elbows, and shoulders. Older dogs sleep 14 to 18 hours a day. The bed is a huge percentage of their life.
- Raise food and water bowls. Elevated feeders reduce the awkward neck-and-shoulder strain of bending to the floor.
- Modify exercise, do not eliminate it. Inactivity worsens OA. Replace long, hard walks with multiple short, gentle ones on soft surfaces. Maintain muscle through swimming or controlled leash walks. Avoid the weekend warrior pattern of one big hike after a sedentary week.
- Keep them warm. Cold and damp worsen arthritis pain. A heated mat, a sweater for outdoor potty breaks in winter, and a draft-free sleeping area all make a difference.
- Manage nails. Long nails change foot mechanics and increase joint stress. Keep them short, ideally with regular Dremel work to avoid the stress of clipping.
- Body harness over neck collar. A well-fitted Y-front harness distributes leash force across the chest rather than the neck and spine, which matters for dogs with cervical or thoracic OA.
When to See Your Vet
Any persistent change in your dog’s mobility deserves a vet visit. Schedule sooner rather than later if you notice any of the following.
- Sudden, severe lameness or refusal to bear weight on a limb. This can indicate cruciate ligament rupture, joint luxation, or other acute injury layered on top of OA.
- Heat, marked swelling, or fever in or around a joint. Septic arthritis and immune-mediated polyarthritis can mimic OA and require completely different treatment.
- Rapid progression of lameness over days to weeks rather than the typical slow decline.
- Loss of appetite, lethargy, or vomiting in a dog on NSAIDs. These can be early signs of gastrointestinal or renal adverse effects and need same-day evaluation.
- Neurological signs, including knuckling, paw dragging, urinary or fecal incontinence, or hind limb weakness. These suggest spinal cord involvement and warrant urgent workup.
- Quality of life declining despite a treatment plan. This is the cue for re-staging, escalating therapy, or discussing whether the current plan is delivering enough relief.
Twice-yearly senior wellness exams catch OA progression earlier than once-yearly visits. Bring a completed LOAD or Helsinki Chronic Pain Index score sheet to every appointment.
Frequently Asked Questions
Can arthritis in dogs be cured?
No. Osteoarthritis is a progressive degenerative disease and the cartilage changes cannot be fully reversed. It can, however, be very well managed. With multimodal treatment, most dogs maintain good mobility and quality of life for years after diagnosis. The realistic goal is slowing progression and controlling pain, not cure.
What is the best pain medication for arthritis in dogs?
The best arthritis medication for dogs depends on disease stage, comorbidities, and individual response. For most dogs with mild to moderate OA, a canine-labeled NSAID (carprofen, meloxicam, deracoxib, firocoxib) or grapiprant is the first-line option. For dogs that do not tolerate NSAIDs or have advanced disease, monthly bedinvetmab injections are increasingly the standard. Gabapentin layers in for breakthrough or neuropathic pain. Your vet will choose based on bloodwork, age, and individual response.
At what age do dogs typically get arthritis?
Clinical signs are most often recognized between five and thirteen years of age, but radiographic changes can begin much earlier. As noted above, nearly 40 percent of dogs aged 8 months to 4 years already show radiographic OA in at least one joint. Early-onset OA is most common in large and giant breeds with developmental orthopedic conditions like hip or elbow dysplasia.
Do glucosamine and chondroitin actually work for dogs?
The evidence is mixed. Some studies show modest improvements, others show no significant benefit over placebo. The safety profile is excellent and many vets still suggest a trial of 60 to 90 days. If your dog shows improvement, continue. If not, do not pour money into it. Omega-3 fatty acids have substantially stronger clinical evidence and should be the first supplement considered.
How much does it cost to treat arthritis in a dog?
Costs vary widely. A diagnostic workup typically runs $200 to $600 including radiographs. Monthly costs for ongoing care can range from $30 to $50 for an NSAID plus omega-3s, up to $150 to $250 per month if bedinvetmab and adjunctive medications are added. Physical rehabilitation sessions typically run $75 to $150 each. The most cost-effective single intervention remains weight loss for overweight dogs, which often reduces medication needs.
Is it safe to give my dog human ibuprofen or aspirin for arthritis?
No. Human NSAIDs including ibuprofen, naproxen, and aspirin can cause serious gastrointestinal ulceration, kidney injury, and death in dogs. Even baby aspirin is not appropriate without veterinary guidance. Always use canine-labeled NSAIDs prescribed by your vet.
Will my dog need surgery for arthritis?
Most arthritic dogs are managed medically without surgery. Surgical options like total hip replacement, femoral head ostectomy, or arthrodesis are reserved for specific situations, including end-stage hip OA in young large-breed dogs, severe elbow OA refractory to medical management, or salvage scenarios. Your vet or veterinary surgeon will discuss surgical candidacy if and when it becomes appropriate.
How do I know if my dog’s arthritis pain is getting worse?
Use a standardized pain scoring tool every month or two. The Liverpool LOAD scale and the Helsinki Chronic Pain Index are both designed for owners to complete at home. Track scores over time. Watch for new behavioral changes: increased reluctance to move, new irritability, changes in appetite or sleep, more time spent isolated. Trends matter more than single scores. Bring the data to your vet so treatment can be adjusted before the dog loses significant function.
RELATED POSTS
View all

Fish Oil for Dogs: Benefits, Dosage by Weight, and What the Research Actually Shows
December 22, 2023 | by seniorsniffs.com

Hip Dysplasia in Dogs: Causes, Symptoms, and the Best Treatment Options
December 22, 2023 | by seniorsniffs.com
